2021 COVID Forecast Update: April
Facts & Forecasts:
On March 1st, we had 514,404 deaths from COVID. The Briggs-3 model predicted 547,006 deaths as of the end of the month – or 32,602 incremental deaths. We ended the month with 551,638 (37,234) . This is within the range of the Briggs-3 forecast, but the forecast was about 12% lower than actual deaths. The Briggs-3 model outperformed the IHME model, which forecast 545,136 as its projection, which is off by 17%.
Overall, looking at absolute difference between each monthly projection since November, the 30 day forecast for Briggs-3 has averaged within 95% of actual. The IHME has averaged 86% of actual.
In terms of the 90 day forecast, that is, forecasts made at the start of January, when there were 347,956 deaths, the actual incremental deaths was 203,682. The Briggs-3 forecast 577,886 (229,930 incremental), and is over by 13% while the IHME forecast 566,479 (218,523 incremental) and was over by 7%. Both models were within forecast range.
Overall, looking at absolute difference between each monthly projection since November, the 90 day forecast for Briggs-3 has averaged within 86% of actual. The IHME has averaged 72% of actual.
Looking Forward:
The 30 day Briggs-3 forecast for April 30, 2021 is 577,938 (30,932 incremental). IHME is very close, with 574,744 (29,608 incremental).
Looking forward 90 days, The forecast for June 30th is 602,712 for Briggs-3 (an incremental 51,074). IHME forecasts 600,053 (48,415 incremental). These forecasts are remarkably close.
For Briggs-3, the year-end forecast is 626,577. This is a reduction from last month’s forecast and is much closer to the original 2021 forecast of 601,000 from November 2020. That said, there are risks that we could trend back upward if vaccinations stall or are ineffective against variants.
The reason for the significant drop in deaths for the Briggs-3 forecast is that the 65+ population has already reached 75% vaccination rate for first dose and 50% are fully vaccinated. The Briggs-3 model expected 50% to be reached on May 10th, and 75% to reached toward the end of the year. Given the 3 to 4 week interval to the second dose, and a minor drop off from first to second dose, we can expect to reach 75% by mid-year. Moreover, the Briggs-3 model had a “best case” of 85% of 65+ fully vaccinated by the end of the year, and if we were to reach this 85% level, the model predicted a little more than 130,000 incremental lives saved compared to the 75% level. Let’s do everything we can to help those most at risk to get fully vaccinated. It can make a huge difference in lives saved.
The reason the vaccination rate of 65+ is so important to the model prediction is 65+ have represented 80% of all deaths thus far. They are nearly 100x more likely to die of COVID compared to someone under 45. With a high vaccination rate, the Infection Fatality Rate (IFR) will drop in half. Last night, I ran the CDC’s reported 29.4% of those under 65 and 73.4% of 65+ receiving at least one shot, and my initial calculations are a halving of the fatality rate over the next month. By the end of April, we should see if the Case Fatality Rates (CFR) drop to about 1%, down from 1.7% over most of the last year. By early May, we could expect the CFR rate to settle at about 0.9% . If so, the accelerated vaccination of 65+ will have saved an incremental 50,000 lives compared to what my model expected.
The Briggs-3 models shows more lives are now being saved by the incremental vaccines than are lost to the disease. As of today, the model calculates 759,254 deaths averted due to vaccinations. The fact that we are only four months into vaccinations and more lives have been saved due to people taking responsibility and action to get vaccinated than have been lost to COVID-19 is inspiring.
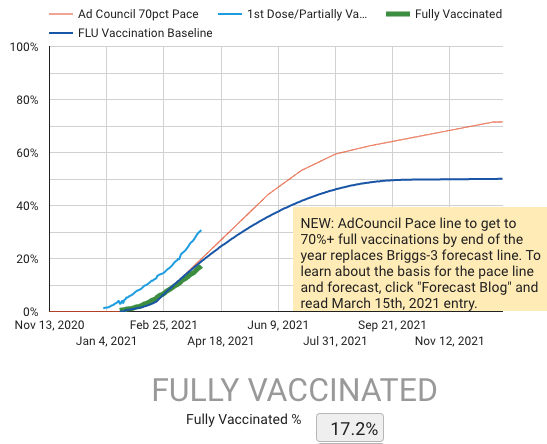
The Briggs-3 model does expect vaccinations to slow as the US approaches 45 to 50% of total US population. The forecast vaccination curve is informed by pattern of flu vaccinations by month. To read more about this forecast, see the forecast blog, link of the bottom left of dashboard. The Briggs-3 model includes public health communications from organizations like the Ad Council that are making a great effort to get the facts out. These PSAs could increase the vaccination rate by 20% to 40% over baseline.
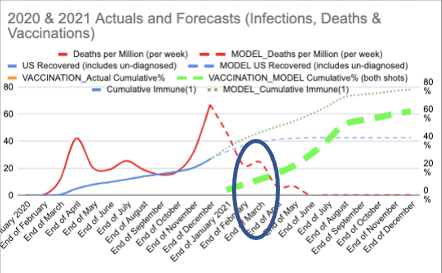
We are not out of the woods yet. The recent uptick in cases and deaths is unfortunate but was predicted back in the November model (see circled portion of chart, showing trend in COVID deaths per million).
The predictable pattern is that any major holiday (in this case, Spring Break and Easter) leads to an uptick in cases and deaths because too many Americans relax social distancing and mask precautions. The Briggs-3 model expected to see a higher vaccination rate among 65+ compared to younger cohorts, and therefore a predictable shift in who is infected. Now that much of the 65+ population has had the opportunity to be vaccinated (and 75% have gotten at least one jab), it will be important for the younger population to be vaccinated to effectively end the pandemic in the US. Those under 45 are expected to be vaccinated at a lower rate than the overall population, and this can be problematic because this age cohort has had a larger role in spreading the virus.
Similar to IHME, which has a current projection and worst case model, there is a “worst case scenario” called Briggs-3.1. Europe is in the 3.1 worst case scenario now, due to slower than forecast vaccinations and the spread of more dangerous variants. It is still possible for Europe to catch up on vaccinations and see an effective end to the pandemic in Q3 (late Q3), but the incremental death toll due to slow vaccinations is projected well above a hundred thousand.
In the US, back in January, due to slow vaccinations and the spread of dangerous variants, the US was trending toward this same worst case scenario. However, By the end of February, the US quadrupled vaccination rates and got back on track. In particular, the vaccination rates among 65+ were outstanding. Therefore, the forecast for the US to see an effective end to the pandemic in early Q3, as originally forecast in November is on track. (You can see the original Research World Article here).
To track the progress of vaccinations in the US, see www.speakerrex.com/dash.html and click on vaccinations to page through the charts and data.
Observations & Commentary:
There is an uptick in cases and deaths from COVID recently. But this recent uptick will not translate into nearly as many deaths as other holidays because vaccinations of 65+ is ahead of forecast. The US will exceed 75% of 65+ partially vaccinated within the next week. The US has already crossed the 50% mark for 65+ fully vaccinated yesterday.
Recall that 65+ accounted for 80% of deaths over the last year. Therefore, I’ll give the unvaccinated 65+ a provocative name of the “Death Pool.”
The death pool shrank from 55 million (the total population in the US that is 65 and older) at the beginning of the pandemic to a little less than 10 million today (9.24 million). Those that remain in the death pool are those not yet vaccinated, minus my calculation of those likely infected with some level of natural immunity.
For those 65+ that remain unvaccinated, the risk of infection, hospitalization and death remains high. 1.94% is the risk of death if infected. That is 1 in 50 have the risk of dying if they are infected with SARS-CoV-2. Keep in mind, the infected number is about 4x higher than the confirmed cases.
The math of the Death Pool is worth considering.
If every person in the Death Pool became infected, we’d expect about 180,000 deaths among the 65+. But, I wouldn’t expect all to become infected. Those not yet infected have managed to avoid infection to date based on a combination of the communities behavior of wearing masks and social distancing, and their own behavior – perhaps minimizing unsafe behaviors. Therefore, instead of an attack rate of 100%, if the attack rate is 50% for this population over the remainder of the year, then we’d expect less than 100,000 incremental deaths among the 65%. Those are horrible odds – basically 1 in 100 of the 65+ not vaccinated could die. But the math is a bit more complex because vaccinations of those people around you make a big difference. The current Briggs-3 model now expects only about 75,000 incremental deaths because there is an expectation of a level of herd immunity that will significantly slow the spread of the virus. The odds of death for those 65+ may drop from 1 in 125 over the past (we’ve lost 440,400 people 65+ which is 1 our of every 125 people 65+) to 1 in about 200 among those not vaccinated. Still, those are terrible odds considering a vaccination changes the odds to far less than 1 in 20,000.
That said, some will refuse to be vaccinated. In a somewhat predictable turn of events, Republicans went from being more likely to get vaccinated early on in the cycle (when Trump was President) to being significantly less likely to get vaccinated now that he isn’t. It seems Republicans shifted from protecting themselves and doing their patriotic duty to defend this county from death and destruction by getting vaccine, to “no thanks.”
It is a similar turn of events to Republicans going from 68% trust in elections before Trump and his made false claims about stolen elections tanked the numbers of republicans with trust in elections to less than 35% (see Morning Consult polling trends). What changed the perception of voting process and integrity wasn’t the facts. What changed was the misinformation in the echo chamber of conservative social media.
My concern for the Republicans in my family and life that I care about is the disease of lies has life and death consequences. The misinformation about the vaccine has life and death consequences. Tens of thousands of unvaccinated people will needlessly die between now and the end of the year. Worse still, hundreds of thousands of unvaccinated people will get infected and infect others, leading to the needless death of fellow citizens.
The challenge is that the recipient of the misinformation may have genuine distrust for government and medical community. How can we engage that person? Pointing out that by not getting vaccinated they’ve got a 1 in 200 chance of dying of COVID and they are contributing the death of others probably isn’t going to lead to a productive conversation. Does it matter to conservatives that FOX News media magnate Rupert Murdoch and former President Trump both were vaccinated make any difference? Once someone has gone down the misinformation rabbit hole, can we drop any type of rope down to help them climb out? Can the misinformation be undone? I wish I knew the answer.
To add some specifics to the magnitude of the problem, the correlation of first dose vaccines by the State’s vote margin for Trump in the 2020 election is now a negative .42. In other words, where Trump won by the most, there is a significantly lower level of vaccinations. This means that these folks are not only more likely to die of COVID-19 in 2021, they are more likely to spread the virus because there are fewer vaccinated people to slow the spread.
The magnitude of the problem is similar for Black Americans. There is a negative .44 correlation. In states with a higher Black American population, there are much lower vaccination rates.
Since last month, Hispanic Americans have stepped up their vaccination rate. They went from negative .09 to positive .05 as of earlier this week. That’s good news.
I am seeing some indications in polling data that Black Americans are more likely to change their stance on vaccines. As Black Americans see so many others successfully vaccinated with limited side effects, it is changing the trend. From my perspective, given the history, we should be doing more to bring vaccinations and vaccine information from trusted sources into Black American communities. Consider Detroit, and the rural areas around Detroit that experiencing a surge in cases. Are we doing enough?
As noted last month, High School Education attainment remains an important demarcation – those with less than a HS degree have a negative correlation of .36 with first dose. That is a little bit better than last month of negative .39, but not by much. This may be related to the complexity in scheduling an appointment, and flexibility in schedule. The skill to find vaccines through online searches, and the luxury of time to get them, the transportation to get to where the vaccines are available work against those with less than a HS degree and less affluence. In addition, those with less than a HS degree are also more likely to have already had COVID, and they may reason they do not need to get the vaccine – or at least they will wait longer before getting the vaccine. The medical research I've read shows it is best for those with COVID to get at least one jab, as the vaccine induced immunity produces in the neighborhood of 30 times more protective antibodies. Therefore, I hope we will see an increased vaccination rate among this population over the next few months.
In areas where there are more vaccinations, I am seeing a negative correlation with deaths (-0.26 after second dose), which is as expected. However, I also observed an increase in cases (0.21 after second dose and 0.37 after the first dose). This correlation was not expected.
The medical research from Israel, the UK and even recently released data from Washington state shows that vaccinations reduce the likelihood of getting infected, so we should see infections trend downward. It isn’t that the vaccinated people are driving this number up. The data from Washington state shows a mere 102 positive cases out of over 50,000 since February 1 are from fully vaccinated people. Considering more than 10% were vaccinated, if vaccines increased the risk, then the number of those vaccinated that were also infected would have exceeded 5,000 – but again, it was just 102.
So what explains the positive correlation in vaccinations and new cases?
I think we are prematurely letting our guard down. Texas, are you listening? You’ve got one of the lowest rates of vaccination in the country.
It is more than just the conservative states -- it is in our own vaccinated households. In my household, after my wife and I got our first dose, I recall being more lenient on my boys meeting up with their friends about 10 days after the first jab. I think my boys only asked to see their friends for dinner because they knew it had been almost two weeks since I had my first vaccine shot. They have been incredibly respectful of the boundaries we set early in the pandemic as a family, and now that both my wife and I had our first shot, I suspect they feel they were putting us at less risk now. While it was a small marginal change in behavior, if we multiply this pattern across millions of people, it produces the uptick in infections that fits the data. The lesson is, we are not out of the woods yet. While there is a psychological relief in getting the first jab, the real physical relief comes two weeks after being fully vaccinated. For me, with Moderna, that is a full six weeks after the initial jab. We need to learn this lesson from the data and be very cautious (and encourage those around us to be cautious) until a full two weeks after FULL vaccination.
The dynamic to consider with the uptick in cases is that it is more pronounced among the younger population. We’ve known since the Lancet study in July and the Oxford study in September that younger people were far more likely to become infected and spread the virus. The CDC cited the Oxford study and showed 18-49 were twice as likely as someone 65+ to become infected. This ratio will become even more tilted toward the younger population as more 65+ become vaccinated and are therefore less susceptible to infection. It should cause the infection fatality rate to drop in half, from 0.4% to 0.2% based on my analysis of CDC data by age. Case Fatality Rate should fall in a similar proportion – from the 1.7% it has been averaging for months to somewhere around 0.9%.
However, the death toll alone may not tell the whole story. The concern, as a father of twin 18 year old boys, is that we don’t know all the longer-term effects of being infected with COVID. We have enough evidence to know that is very rare for it to lead to death in a healthy younger person, but it can be damaging to their health. Vaccinations among young people can protect the overall population from the spread a variants and further mutations, as well as protect the young person from uncertain COVID outcomes.
Recommendations:
I suspect most reading this post will already be vaccinated. Right on! Consider if you can help others to get vaccinated. Maybe it is helping make an appointment. Maybe it is helping to arrange transportation. Maybe it is helping get answers (Ad Council’s “It’s Up To You” site is a great place to start). If you’ve been vaccinated, keep your guard up until a full two weeks after the second dose, and encourage other family members to do the same. Look outside the US and consider how we might help others around the world to get vaccinated sooner. This is a global fight.
We certainly have done a lot to reduce the death toll in the US, and we should be asking how we can help save lives globally. Besides valuing lives beyond our borders, helping with global vaccination is in our interest in protecting ourselves and our families. As long as the virus is spreading it has the risk of mutating. There is already evidence that some of the strains are more infectious and potentially more deadly. Now that we have effective vaccines, we are in a race against the virus. It’s up to us to end this.
For more information on the model, click on the dashboard and select Model Methodology at the bottom left.
Related Analysis
- 3 March, 2021:
March 2021 Update
- 28 April 2020:
Guns, Germs And Beer. Four Phases of the Economy
- 2 April 2020:
The Math Of Why Herd Immunity Isn't Viable in 2020